
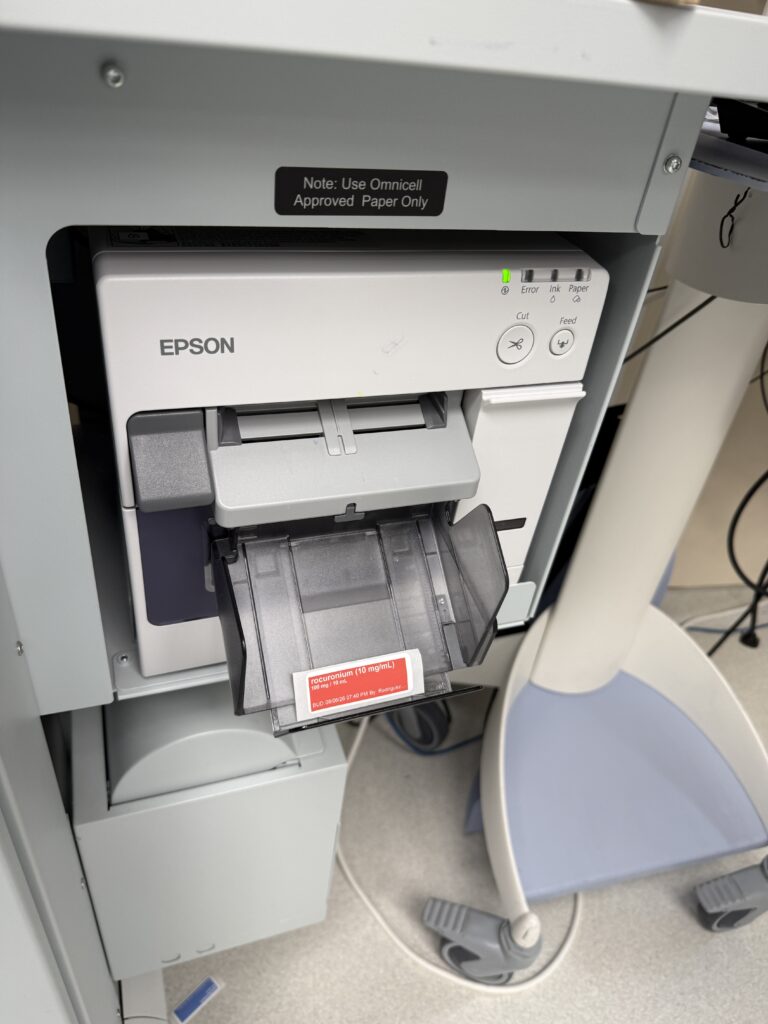
Our pharmacy recently transitioned the printers for our automated drug dispensing cabinets from Codonics to Epson. Of the many flaws of this “new” printer, the flimsy label catch bin is quite a pain in the butt. In the busy OR space behind the curtain, the slightest bump knocked the bin to the floor. After a month of use, a third of the catch bins had been broken or lost from the constant collisions.
THE PROBLEM
The factory produced catch bin relies on small flimsy tabs to hold it in place. Perhaps the design was meant to prevent damage when a force was applied, but the tabs are so loose as to render the bin useless.
DESIGNING A BETTER PRODUCT
This is what I call a “lunch break” project; something that can be designed quickly on an OR lunch break and sent to my 3D printer before heading back to the OR.
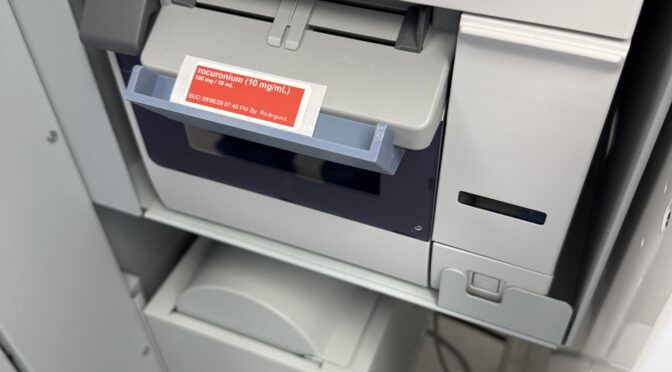
I measured the label printer and came up with a simple design with a much smaller footprint and tighter fitting tabs. Typically, at most, 4-5 labels would be printed at a time, so a very small footprint would suffice for the catch bin. With the small footprint, the risk of bumping into it would be lower and thus a tighter fit would be less of a worry (assuming that’s why the manufacture designed the OEM catch bin as it was).
Here is the CAD design of the project:
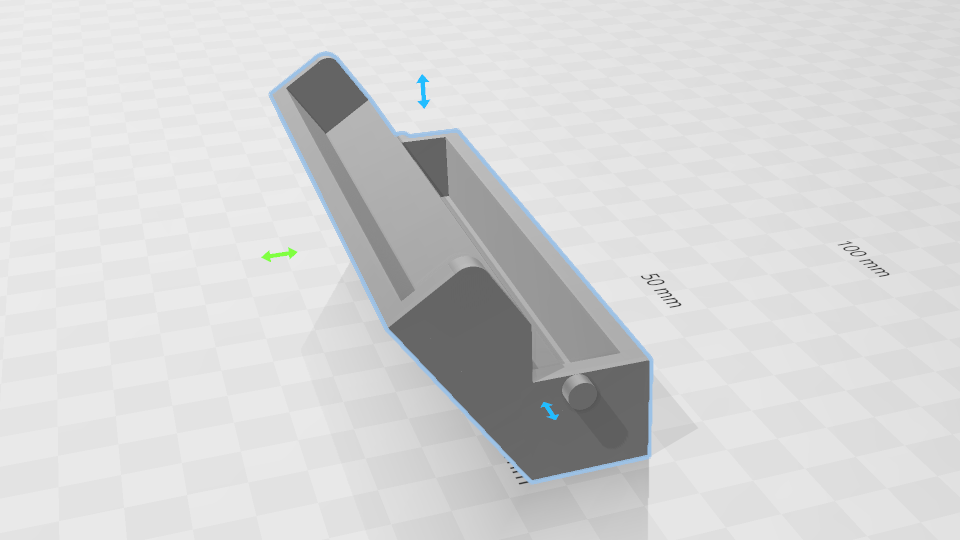
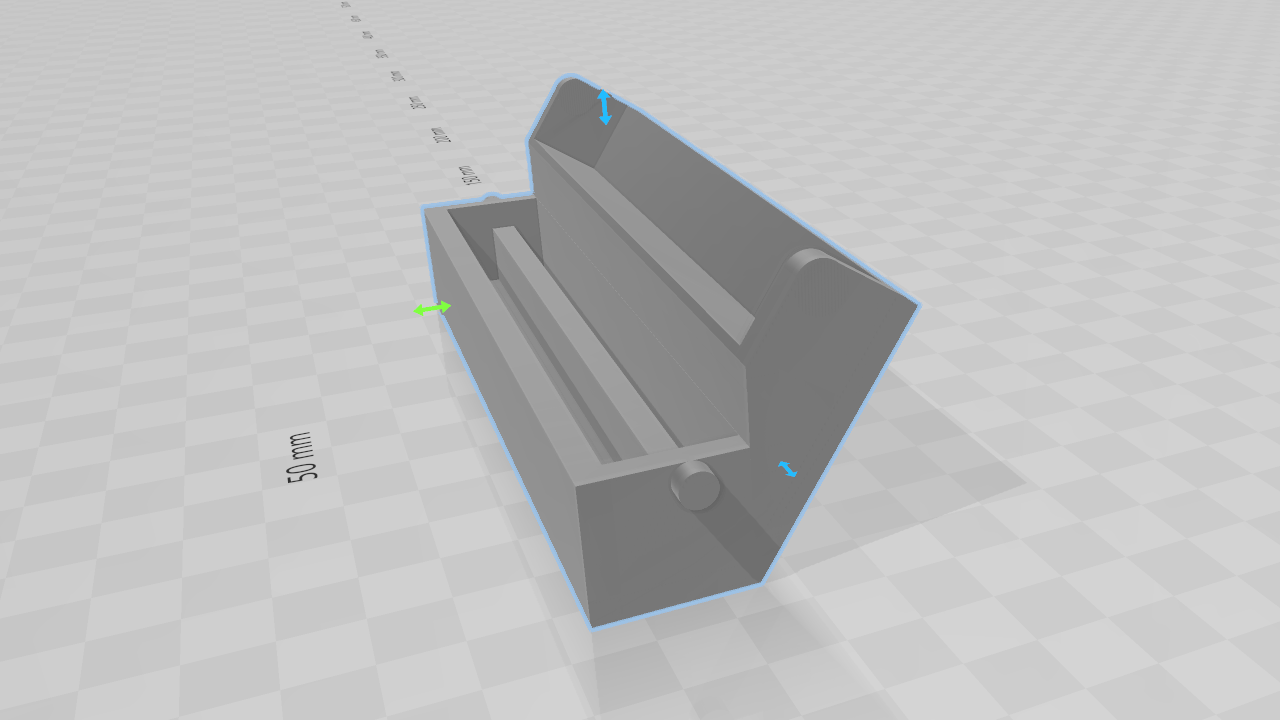
I sliced the model at 0.28 mm layer height for quick 3D printing and printed the model on a Bambu Labs P1S in inexpensive CC3D Blue-Gray PETG. The model weighs 37g and costs 55 cents. With our current inventory of 22 of theses label printers, and with some prototypes printed, the full cost of implementing this project was approximately $14.
THE RESULT
After vetting two of the models in a couple ORs over a week, the feedback for very positive. Over the next week I implemented the label catch into all of the ORs.

I started implementing this project about 8 months ago and all of the label catches are still intact and fully functional. I have continued to receive frequent feedback about how this project has improved OR workflow.
This project is an excellent example of where 3D printing shines in medicine. The manufacturer of the printer, Epson, failed to account for real world implementation of their product and continued to fail with lack of post-market surveys to confirm proper functionality of their product.
Additionally, this project highlights how easy any clinician can immediately improve their working environment with 3D printing. This CAD model is composed of simple geometric shapes, which does not require advanced CAD modeling experience and the model was printed on an inexpensive consumer 3D printer.
If you’re are dealing with the same problem, you can download my STL for this project and print it yourself here: Printables
















































